Address Change for Mailed Claims Submissions (EFFECTIVE 6/30/23) Please submit claims by mail to Partners Health Plan | P.O. Box 240356 | Apple Valley, MN 55124
Submit a Claim
To ensure prompt adjudication, please remember to send all claims to PHP using one of the following options:
By Mail:
Effective 6/30/23 - Please submit claims by mail to: Partners Health Plan P.O. Box 240356 Apple Valley, MN 55124
Electronic Submission:
Options for electronic claims submission
PHP’s Submitter ID is 14966
HealthSmart Clearinghouse – CareVu
If you’d like to establish a connection directly with CareVu, please complete the EDI Enrollment Packet.
For more information, you can contact CareVu at: 888-744-6638
Optum
866-678-8646
Other Clearinghouses
Select Optum
Web-based Claims Submission:
Providers can now easily create and upload a professional or institutional single claim as a pdf file via the provider portal (php.healthsmart.com). Please note that only 1 claim should be uploaded per PDF.
Web-based claims are considered paper claims and will follow all existing claim submission protocols.
Please note that onlyvalid claim forms (CMS 1500 or UB 04)may be uploaded using this method.
PHP would like to remind our providers of the ease of establishing and submitting claims electronically.In addition, we would like to also remind everyone to regularly confirm with their billing service (Clearinghouse) that all electronic submissions have been successfully transmitted and received. If the claim is not successfully transmitted, there will be delays in PHP’s ability to adjudicate the claims on a timely basis. Please check all error logs and resubmit the claim accordingly – timely filing rules still apply for resubmissions.
Balance Billing is not Permitted: Please be reminded that under New York State Law, a Provider participating in the Medicaid program, or a Medicaid Managed Care plan, is prohibited from requesting any monetary compensation from a Medicaid beneficiary, or their responsible relative. In addition, a Medicaid beneficiary, including a Medicaid managed care member, must not be referred to a collection agency for collection of unpaid medical bills or otherwise billed.
The Partners Health Plan Network Development and Provider Relations team is here to assist you with your billing, claims, authorization, education, and any other general inquiry. Use the Contact Us button below to complete a Provider Ticket Submission Form.
Resources, guidelines and information needed to request Durable Medical Equipment and Prosthetics / Orthotics.
The DME Team accepts, reviews, follows up on, processes, and completes all DMEPOS requests.
Phone: (646) 455-1594 | Fax: (646) 948-1027 Email:This email address is being protected from spambots. You need JavaScript enabled to view it.
All DMEPOS requests require Prior Approval (PA); no verbal approval is allowed. PA is not required for Continuity of Care
Required Clinical Paperwork
Prescription or Physician’s Written Order is required for new DMEPOS requests (see exceptions in Product Categories Guidelines). Additional clinical justification may be requested if required by CMS, Medicaid, and/or PHP guidelines:
Prescription/Physician’s Written Order with the member’s first and last name, date of birth, valid ICD-10 diagnosis code(s), ordering physician’s name and license/NPI number.
Should clearly state the item(s) name, quantity, and, if applicable, size, length of needs or number of refills.
Should be signed and dated within three months from the request date.
E-signature is accepted.
Physician’s name and date cannot be stamped if on prescription pad.
Chart or Progress Notes with the member’s first and last name, date of birth, date of encounter; ordering physician’s name and license/NPI number:
Must provide clinical justification for the requested item(s).
Must be dated within the CMS/Medicaid approved timeframe for the requested item(s).
Letter of Medical Necessity (LMN) with the member’s first and last name, date of birth, date of encounter; ordering physician’s name and license/NPI number.
Must provide clinical justification for the requested item(s).
Must be dated within the CMS/Medicaid approved timeframe for the requested item(s).
For your convenience, PHP has developed fillable templates to assist in expediting the LMN approval process. Use the links below to download the fillable templates.
Item is being furnished by a physician or treating practitioner during an office visit where the provider determines that the brace is needed immediately due to medical necessity, or
Item is being furnished by an occupational therapist or physical therapist who determines that the brace needs to be furnished as part of a therapy session(s).
This applies to the following HCPCS codes: L0648, L0650, L1832, L1833, and L1851.
If dispensed by a DME vendor, this vendor must submit the request for a post-date authorization to DME Department shortly after the service date.
All standard requests for DMEPOS are authorized within three business days of receipt of a clean PA request.
All expedited requests for DMEPOS are authorized within 24 hours of receipt of a clean PA request.
Prescription or Physician’s Written Order should specify the type of the lift (i.e., hoyer/hydraulic, manual, power) and sling if other than the standard (i.e., with the commode opening); should have either member’s height and weight or size of the sling.
Chart notes OR Letter of Medical Necessity should justify the medical need per Medicare requirements below:
A patient lift is covered if transfer between bed and a chair, wheelchair, or commode is required and, without the use of a lift, the beneficiary would be bed confined.
Replacement Sling for Patient Lift
Required:
Prescription or Physician’s Written Order for Replacement sling for the patient lift indicate the requested sling type.
Hospital beds
Required:
Prescription or Physician’s Written Order should specify the type of bed, rails (half or full length), and required type of support surface (i.e., gel overlay or APP).
Chart notes OR Letter of Medical Necessity should justify the medical need per Medicare requirements.
General hospital bed requirements (at least one of the requirements should be met):
The beneficiary has a medical condition which requires positioning of the body in ways not feasible with an ordinary bed. Elevation of the head/upper body less than 30 degrees does not usually require the use of a hospital bed, or
The beneficiary requires positioning of the body in ways not feasible with an ordinary bed in order to alleviate pain, or
The beneficiary requires the head of the bed to be elevated more than 30 degrees most of the time due to congestive heart failure, chronic pulmonary disease, or problems with aspiration, or
The beneficiary requires traction equipment, which can only be attached to a hospital bed.
A variable height hospital bed is covered if the beneficiary meets one of the general requirements and requires a bed height different than a fixed height hospital bed to permit transfers to chair, wheelchair or standing position.
A semi-electric hospital bed is covered if the beneficiary meets one of the general requirements and requires frequent changes in body position and/or has an immediate need for a change in body position.
A heavy duty extra wide hospital bed is covered if the beneficiary meets one of the general requirements and the beneficiary's weight is more than 350 pounds, but does not exceed 600 pounds.
An extra heavy-duty hospital bed is covered if the beneficiary meets one of the general requirements and the beneficiary's weight exceeds 600 pounds.
A total electric hospital bed is not covered; the height adjustment feature is a convenience feature. Total electric beds will be denied as not reasonable and necessary.
Air Loss Mattress
Required:
Prescription or Physician’s Written Order.
Chart notes OR Letter of Medical Necessity should justify the medical need per Medicare requirements.
Air Loss Mattress is covered if the beneficiary meets at least one of the following three Criteria (1, 2 or 3):
The beneficiary has multiple stage II pressure ulcers located on the trunk or pelvis which have failed to improve over the past month, during which time the beneficiary has been on a comprehensive ulcer treatment program including each of the following:
Use of an appropriate group1 support surface, and
Regular assessment by a nurse, practitioner, or other licensed healthcare practitioner, and
Appropriate turning and positioning, and
Appropriate wound care, and
Appropriate management of moisture/incontinence, and
Nutritional assessment and intervention consistent with the overall plan of care
The beneficiary has large or multiple stage III or IV pressure ulcer(s) on the trunk or pelvis.
The beneficiary had a myocutaneous flap or skin graft for a pressure ulcer on the trunk or pelvis within the past 60 days, and has been on a group 2 or 3 support surface immediately prior to discharge from a hospital or nursing facility within the past 30 days.
Ambulation devices: Cane / Walker / walker with seat (rollator)
Required:
Prescription or Physician’s Written Order.
Replacement: Prescription is not required for one replacement after at least one year of use.
Standard Wheelchair
Required:
Prescription or Physician’s Written Order should specify the type of the wheelchair (standard manual, lightweight, heavy-duty) and weight for heavy-duty wheelchairs.
Chart notes OR Letter of Medical Necessity should justify the medical need per Medicare requirements.
A manual wheelchair for use inside the home is covered if:
The member has a mobility limitation that significantly impairs his/her ability to participate in one or more mobility-related activities of daily living (MRADLs) such as toileting, feeding, dressing, grooming, and bathing in customary locations in the home.
The member has sufficient upper extremity function and other physical and mental capabilities needed to safely self-propel the manual wheelchair, or
The member has a caregiver who is available, willing, and able to provide assistance with the wheelchair.
By signing the letter of medical necessity, the ordering physician also acknowledges that the following is true:
The residence provides adequate access between rooms for use of the manual wheelchair.
The member has not expressed an unwillingness to use the manual wheelchair that is provided in the home.
Heavy-duty / extra heavy-duty wheelchairs
A heavy-duty wheelchair is covered if the member weighs more than 250 pounds or the member has severe spasticity.
An extra heavy-duty wheelchair is covered if the member weighs more than 300 pounds.
PHP allows the use of both wheelchair for longer distances and walker/rollator for inside the home.
Replacement: Prescription is not required for one replacement of shower chair after at least two years of use.
[fa6-solid--wheelchair]
Custom-Made DME (manual and power mobility)
All requests must be referred to the specialized clinic for custom wheelchairs/DME prior to submitting it to PHP for approval.
Positioning shower/commode chair
Medicaid Requirements:
A positioning bath chair is covered when the documented medical and hygiene needs of the member require proper positioning and alignment while providing a stable and safe means of support during bathing. Included are all accessories required for positioning of the member such as but not limited to a head support, trunk laterals, hip laterals, pelvic belt or chest belt.
Reclining shower/commode chair
Medicaid Requirements:
Reclining shower-commode chair is covered when recline is necessary to complete hygiene needs, and the member either has positioning needs that cannot be met by upright and a fixed angle chair or the member’s postural control requires recline.
Rehab (self-propelling) shower/commode chair
Medicaid Requirements:
Rehab (self-propelling) shower/commode chairs are defined as chairs that have large rear wheelchair style wheels, typically 18 inches or greater, to allow for self-propulsion.
Rehab style chairs are covered when the member has access to a roll in shower and is capable of independently propelling the chair into the shower and independently completing all aspects of the shower routine.
Custom Manual Wheelchair
Medicare Requirements:
A custom manual wheelchair is covered if, in addition to the general coverage criteria above, the specific configuration required to address the member’s physical and/or functional deficits cannot be met using one of the standard manual wheelchair bases plus an appropriate combination of wheelchair seating systems, cushions, options or accessories (prefabricated or custom fabricated), such that the individual construction of a unique individual manual wheelchair base is required.
A custom manual wheelchair is not reasonable and necessary if the expected duration of need is less than three months (e.g., post-operative recovery).
Manual Wheelchair With Tilt in Space
Medicare Requirements:
A manual wheelchair with tilt in space is covered if the member meets the general coverage criteria for a manual wheelchair above, and if criteria (1) and (2) are met:
The member must have a specialty evaluation that was performed by a licensed/certified medical professional (LCMP), such as a PT or OT, or physician who has specific training and experience in rehabilitation wheelchair evaluations and that documents the medical necessity for the wheelchair and its special features (see Documentation Requirements section). The LCMP may have no financial relationship with the supplier.
The wheelchair is provided by a Rehabilitative Technology Supplier (RTS) that employs a RESNA-certified Assistive Technology Professional (ATP) who specializes in wheelchairs and who has direct, in-person involvement in the wheelchair selection for the patient.
[fa6-solid--lungs]
Respiratory Equipment and Supplies
PAP Machine and Supplies
Required for initial set-up:
Prescription or Physician’s Written Order should specify the type of PAP machine (e.g., CPAP, BiPAP, APAP).
Chart notes with in-person clinical evaluation by the treating practitioner prior to the sleep test to assess the member for obstructive sleep apnea.
Sleep study test ordered by the treating practitioner.
There is a three-month trial period after which the prescribing physician must conduct clinical re-evaluation and document that the member is benefiting from PAP therapy to continue using a PAP machine beyond the trial period. It may not require a new appointment; DME vendors usually work with the prescribing physicians directly.
Required for replacement machine:
Prescription or Physician’s Written Order should specify the type of PAP machine.
New sleep study is NOT required.
Required for PAP accessories:
Prescription or Physician’s Written Order for required supplies.
PAP supplies are only ordered on as needed basis for up to three months at a time. Prescribing physician should submit the request for supplies to the DME vendor.
Scripts are valid for 12 months; during this time Member can call a DME vendor requesting supplies as needed.
Oxygen Equipment and Supplies
Required for initial set-up:
Prescription or Physician’s Written Order should indicate the type of oxygen therapy (i.e., Oxygen concentrator, Portable tanks, Home fill-in system, etc), oxygen saturation level, and oxygen flow rate (liter per minute).
Chart notes should justify the need for oxygen therapy and requested type including gas testing results.
CMN (Certification of Medical Necessity) form is retired on 1/1/2023.
Medicare requirements:
Initial coverage of home oxygen therapy and oxygen equipment is reasonable and necessary for Groups I and II if all of the following conditions are met:
The treating practitioner has ordered and evaluated the results of a qualifying blood gas study performed at the time of need; and,
The beneficiary's blood gas study meets Medicare criteria; and,
The qualifying blood gas study was performed by a treating practitioner or by a qualified provider or supplier of laboratory services; and,
The provision of oxygen and oxygen equipment in the home setting will improve the beneficiary’s condition.
Pulse Oximeter
Beneficiaries may self-administer home based overnight oximetry tests under the direction of a Medicare-enrolled Independent Diagnostic Testing Facility (IDTF). A DME supplier or another shipping entity may deliver a pulse oximetry test unit and related technology to a beneficiary’s home under the following circumstances:
The beneficiary’s treating practitioner has contacted the IDTF to order an overnight pulse oximetry test before the test is performed.
The test is performed under the direction and/or instruction of a Medicare-approved IDTF. Because it is the beneficiary who self-administers this test, the IDTF must provide clear written instructions to the beneficiary on proper operation of the test equipment and must include access to the IDTF in order to address other concerns that may arise. The DME supplier may not create this written instruction, provide verbal instructions, answer questions from the beneficiary, apply or demonstrate the application of the testing equipment to the beneficiary, or otherwise participate in the conduct of the test.
The test unit is sealed and tamper-proof such that test results cannot be accessed by anyone other than the IDTF which is responsible for transmitting a test report to the treating practitioner. The DME supplier may use related technology to download test results from the testing unit and transmit those results to the IDTF. In no case may the DME supplier access or manipulate the test results in any form.
Portable Oxygen Systems
A portable oxygen system is covered if the beneficiary is mobile within the home for Groups I and II, and the qualifying blood gas study was performed while at rest (awake) or during exercise. If the only qualifying blood gas study was performed during sleep, portable oxygen will be denied as not reasonable and necessary.
Required for Recertification:
Oxygen therapy must be recertified every 12 months.
Prescription or Physician’s Written Order should indicate the type of oxygen therapy (i.e., Oxygen concentrator, Portable tanks, Home fill-in system, etc), oxygen saturation level, and oxygen flow rate (liter per minute).
Chart notes should justify the need for oxygen therapy.
Maintenance and Oxygen Supplies:
Maintenance of the equipment such as repairs and replacement of parts is included in the monthly rental rate.
Oxygen supplies are included in the monthly rental rate and ordered on as needed basis.
Nebulizer
Required:
Prescription or Physician’s Written Order.
Chart notes OR Letter of Medical Necessity specifying the drug: name and dosage.
[zondicons--travel-walk]
Custom-made Orthotics and Prosthetics
Required:
Prescription or Physician’s Written Order should indicate a custom item is required.
Chart notes OR Letter of Medical Necessity indicating the medical necessity for customization.
[fa6-solid--prescription-bottle-medical]
Enteral Nutrition
Via G-Tube
Coram is the preferred vendor.
Phone: (888) 334 -7978
Fax: (800) 693-7322
Required for initial request:
Prescription or Physician’s Written Order should include the name of formula, dosage, and method of feeding.
Chart notes outlining the nutritionist’s assessment, failed swallow study and G-Tube procedure.
CMN (Certification of Medical Necessity) form is retired on 1/1/2023.
Intake process may take up to seven business days.
Monthly deliveries of formula and supplies
Member must call in requesting new delivery each month.
Coram re-order department phone number: (888) 334-7978.
Oral Intake / Nutritional Drinks (Glucerna, Ensure, special formula for metabolic disorders, etc)
Part B benefit authorized by DME. Do not call in the pharmacy:
Required:
Prescription or Physician’s Written Order should include the name of formula, dosage, method of feeding, and BMI.
Chart notes or Letter of Medical necessity that meets at least one of the coverage criteria below:
Member has inborn metabolic disorder(s).
Member has a chronic disease or medical condition complicated by rapid short-term weight loss, have a permanent structural limitation that prevents the chewing of food, and the placement of a feeding tube is medically contraindicated.
Member has a chronic disease or medical condition complicated by rapid short-term weight loss requiring supplemental nutrition and meets ONE of the following criteria:
Member has a body mass index under 18.5 as defined by the Center for Disease Control and has been in a nutrition program with documented compliance with an appropriate medical nutritional plan of care (up to 1,000 calories per day), or
Member has a body mass index under 22 as defined by the Center for Disease Control and has been in a nutrition program with documented compliance with an appropriate medical nutritional plan of care (up to 1,000 calories per day) and documented, unintentional weight loss of 5 percent or more within the previous 6-month period.
For Members with a diagnosis of HIV, AIDS, or an HIV-related illness, or other disease or condition requiring supplemental nutrition OR who have a chronic disease or medical condition complicated by rapid short term weight loss requiring supplemental nutrition, ONE of the following criteria must be met:
Member has a body mass index under 18.5 and has been in a nutrition program with documented compliance with an appropriate medical nutritional plan of care (up to 1,000 calories per day), or
Member has a body mass index under 22 and has been in a nutrition program with documented compliance with an appropriate medical nutritional plan of care (up to 1,000 calories per day) and documented, unintentional weight loss of 5 percent or more within the previous 6-month period.
CGM is a Part B pharmacy benefit that requires a prior approval from DME. Providers should submit the required paperwork to DME Department for approval. After the request is approved, Member will be able to pick up CGM supplies at the pharmacy.
Available CGM brands:
Dexcom G6 (preferred)
Abbott FreeStyle Libre (non-preferred) has a Step Therapy requirement: Participant must try and fail using Dexcom first except if Member has been using Freestyle Libre system prior to joining PHP.
GCM System Requirements
Required:
Filled and signed PHP CGM request form OR Prescription with a valid ICD-10 diagnosis code and CGM system name. Note: PHP CGM request form, if filled in properly and completely, meets most of the requirements below. Chart notes may compliment the PHP CGM request form.
Chart notes justifying the medical need for CGM system:
Member has type 1, type 2, or gestational (during pregnancy) diabetes (too much sugar in your blood)
Member meets ONE of the following:
Member performs at least 4 finger-stick glucose (blood sugar) tests daily
Member is being treated with insulin and meet ONE of the following:
Member is using a continuous subcutaneous (injection under the skin) insulin infusion pump
Member uses 3 or more injections of insulin daily
Member is on an insulin treatment plan that requires frequent adjustment of insulin dosing
Member meets ALL of the following:
Member has a clinical need that cannot be managed with self-monitoring of blood glucose (such as frequent hypoglycemia [low blood sugar], hypoglycemic unawareness, unable to achieve control of diabetes)
Member has either tried (without adequate results or continuous need is identified by your doctor) or does not have access to a professional continuous glucose monitor from your doctor's office
[fa6-solid--kit-medical]
Medical Supplies
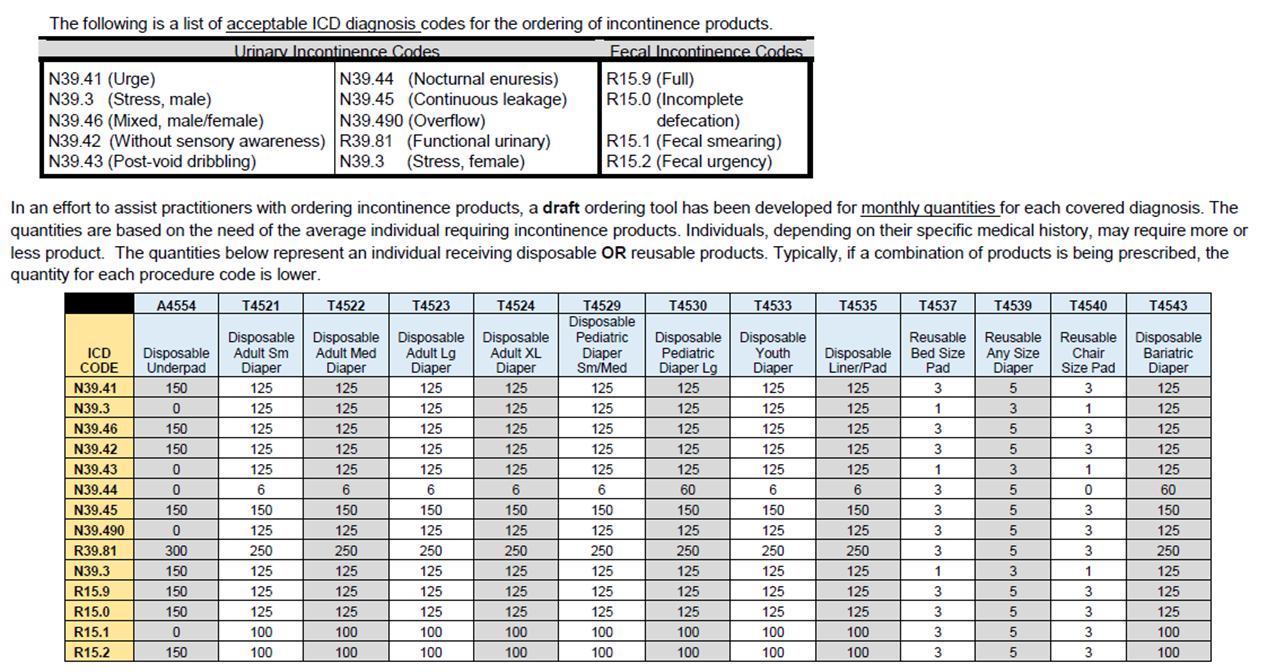
Incontinence supplies
Initial order:
Prescription or Physician’s Written Order with a valid ICD-10 diagnosis code of urinary incontinence is required for the initial order.
Ordering quantity is based on ICD-10 diagnosis of urinary incontinence, see the table below.
Chart notes or LMN required to justify the medical need for ordering quantity above Medicaid limit.
Change in order:
Prescription or Physician’s Written Order and LMN required if the new ordering quantity is above Medicaid limit.
Recertification:
Recertification period: six months.
Clinical paperwork is not required if there is no change in the request.
Wound care supplies
PHP has waived the Prior Approval (PA) requirement for wound care surgical dressings for Par and Non-Par Providers. Providers will be able to deliver and bill for Surgical Dressings based on the prescribing physician’s prescription and clinical notes. PHP continues to require all Providers to follow Medicare and Medicaid requirements for the Surgical Dressing billing and will be conducting semi-annual audit for quality assurance purposes. Please contact PHP’s DME Department at (646) 455-1594 If you have any questions.
Stoma supplies (ostomy/colostomy)
Initial order:
Prescription or Physician’s Written Order with detailed product description: item name, size, reorder number, ordering quantity, number of refills.
Progress or chart notes.
Recertification:
Recertification period: up to 12 months.
Prescription or Physician’s Written Order with detailed product description: item name, size, reorder number, ordering quantity, number of refills.
Suction, Tracheostomy Supplies
Initial order:
Prescription or Physician’s Written Order with detailed product description: item name, size, reorder number, ordering quantity.
Progress or chart notes.
Recertification:
Recertification period: up to 12 months.
Prescription or Physician’s Written Order with detailed product description: item name, size, reorder number, ordering quantity, number of refills.
The Partners Health Plan Network Development and Provider Relations team is here to assist you with your billing, claims, authorization, education, and any other general inquiry. Use the Contact Us button below to complete a Provider Ticket Submission Form.
An individual I support just enrolled with Partners Health Plan (PHP). What do I have to do?
PHP has a 90-day Continuity of Care period when all waiver claims are paid without prior authorization. During first 30 days of enrollment, the member’s assigned Care Manager will contact you to gather the information regarding the services you provide, discuss goals, and invite you to the member’s Life Plan (LP) meeting.
What information do I need to bring to the Life Plan meeting?
You will be expected to discuss any issues related to the member’s employment, goals, and supports needed. You will also have to identify the type of service the member needs (Extensive or Intensive).
How is SEMP authorized?
PHP’s Life Plan serves as a prior authorization of services (Section IV). The Life Plan will include the type of service you are authorized to provide, along with the number of units authorized.
The standard authorization is for a 6-month period. No approval is needed from the DDRO.
Please note that authorizations for individual and group SEMP are grouped into a single authorization and separate authorizations for individual and group services are not necessary.
There is a separate distinction in the coding for Intensive SEMP and Extended SEMP and separate authorizations are necessary.
What if the individual needs more units before the next Life Plan?
Additional units may be requested at any point during the LP cycle. The member’s Care Manager must be notified of your request so they can schedule an Interdisciplinary Team (IDT) meeting to assess the member’s need for additional units.
If the additional services are agreed upon, an addendum to the LP will be completed to reflect changes to the SEMP authorization. The DDRO is not part of PHP’s approval process (no SARF or SAM needed).
What if I provided unauthorized SEMP services?
Any units billed in excess of the authorized units noted in the member’s Life Plan will be denied.
What are my responsibilities if SEMP services change?
The member’s Care Manager must be notified as soon as the member’s services need to change to adjust the authorization accordingly to avoid claim denials (for example: change from Extended to Intensive).
Do I need to wait 45 days to request Intensive SEMP?
No, PHP has the flexibility to waive this requirement.
What about State-Funded SEMP? (ACCES-VR)
This service is not a covered PHP benefit and continues to be funded by the State.
Can you roll over unused units to the next authorization?
No. PHP issues new authorizations every 6 months, with the standard units of 100 hours for Extended and 125 hours for Intensive SEMP.
Where do I go if I have additional questions about billing, claims, and authorizations?
Select DD Agency and Claim or Authorization Issue to ensure your inquiry is routed to the correct team member
Need Provider Assistance?
The Partners Health Plan Network Development and Provider Relations team is here to assist you with your billing, claims, authorization, education, and any other general inquiry. Use the Contact Us button below to complete a Provider Ticket Submission Form.
Partners Health Plan (PHP) has created the PHP Self-Direction (SD) Professional Support Network (PHP-SDSN) as a reflection of commitment to, and belief in, the power and value of self-direction to allow individuals with IDD to have the control and authority over their lives.
Joining the PHP-SDNS provides Self-Direction Professionals (Brokers and Fiscal Intermediaries) a unique package of enhanced benefits for their clients and client prospects and in-network rates that reflect the value of the services you provide to PHP members.
[warning]
Why Join
In addition to the comprehensive care management and IDD-tailored health, dental, vision and hearing benefits already offered to PHP Members, Self-Direction Professionals who join the PHP-SDSN can offer clients who are PHP Members:
Budget Approval
Almost immediate approval of Medicaid budget components and authorization of services
Program Changes
Guaranteed five (5)-day turnaround on budget neutral program changes.
Transportation
Transportation benefits outside of self-direction budget enabling travel to emergent, non-emergent and social events
Monthly Cash Allocation
A monthly cash allocation (via special debit card) for over-the-counter (OTC) health-related purchases (and, in 2004 OTC card use will be extended to utility bill reimbursement).
Rapid Authorization
Rapid authorization of IDD services including but not limited to day hab, comm hab, respite, SEMP and IDGS
Don't take our word for it... Testimonials.
Need Provider Assistance?
The Partners Health Plan Network Development and Provider Relations team is here to assist you with your billing, claims, authorization, education, and any other general inquiry. Use the Contact Us button below to complete a Provider Ticket Submission Form.
Through Self-Direction, individuals with IDD have the freedom to make choices that will help them be active in their community, reach their goals and to live independently.
Under Self-Direction, you can:
Live in the home and community that you choose.
Do things you enjoy such as work, church, or spend time with friends.
Choose services and supports to meet your health and life goals.
The PHP DIfference:Self-Directing With Partners Health Plan
Partners Health Plan (PHP) is health insurance designed just for adults with Intellectual and Developmental Disabilities (IDD) and is committed to supporting its members in Self-Direction. PHP members can combine the benefits of their no-cost health insurance with Self-Direction to reach their goals!
OTC Benefit Card
An easy and flexible way to boost your health and independnece
PHP provides qualified members with $200 a month, outside of their Self-Direction budget, to purchase healthy food, personal care, over-the-counter (OTC) items, and help pay for utitlies.
Transportation Services
Live more independently and get where you need to go!
PHP members can stretch their self-direction budget dollars by using the PHP transportation benefit. They receive transportation, when they need it, where they need it, at no cost.
Comprehensive Medical Benefits and Providers
Meet your health goals!
PHP members enjoy integrated medical benefits that include dental, vision and hearing benefits, and a network of providers with experience supporting people with IDD.
“Self-Direction has given me more freedom and flexibility to do what I want in the community. I wouldn’t have accomplished my childhood dreams if it weren’t for self-direction.”
Jess, PHP Member
Contact us to
learn more!
CALL (855) 747-5483 OR Complete The Form Below
Are you a current PHP member interested in Self-Direction?
Getting started with Self-Direction as a PHP member is easy!
Step 1
Contact your Care Manager to learn more about Self-Direction
Step 2
Select a Support Broker and Fiscal Intermediary to develop a budget to help you manage your money.
Step 3
Start self-directing!
Connect with our outreach team to learn more about the PHP Care Complete FIDA-IDD Plan!
You can reach out to one of our NYS licensed Outreach Associates to schedule a one on one education session at your convenience.
Are you ready to enroll in PHP Care Complete FIDA-IDD Plan?
To enroll, visit or call NY Medicaid Choice at 1-844-343-2433 (TTY: 1-888-329-1541), Monday through Friday, 8:30 AM to 8:00 PM, and Saturday, 10:00 AM to 6:00 PM.
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.
Click the link above to continue or click outside of the box to CANCEL
You are now leaving Partners Health Plan
Partners Health Plan provides links to web sites of other organizations in order to provide visitors with certain information. A link does not constitute an endorsement of content, viewpoint, policies, products or services of that web site. Once you link to another web site not maintained by Partners Health Plan, you are subject to the terms and conditions of that web site, including but not limited to its privacy policy.